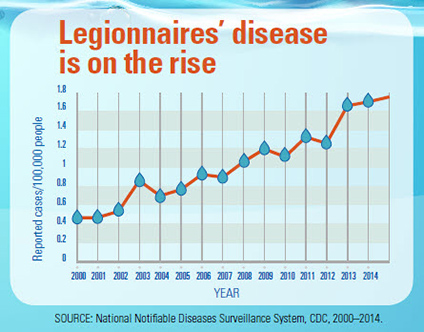
 What do you think is the primary reason Legionnaires’ disease has not decreased since the outbreak in Philadelphia — 43 years ago this week — that led to its discovery?
What do you think is the primary reason Legionnaires’ disease has not decreased since the outbreak in Philadelphia — 43 years ago this week — that led to its discovery?
A. Agreement on a strategy for preventing Legionnaires’ disease has not been reached.
B. Information, services, and technologies needed to control Legionella in building water systems are not available to building owners and managers.
C. Building owners and managers have not implemented the information, services, and technologies available to them to control Legionella in building water systems.
“A” is not true. Since the early 1980s, scientists have agreed, based on several studies, that Legionnaires’ disease is caused by Legionella bacteria emitted from cooling towers, plumbing (domestic/potable) systems, whirlpool spas, and other water-related equipment in buildings.
In the 1990s, several governments and industry groups released official statements that managing building water systems to minimize Legionella is the best strategy for reducing the risk of Legionnaires’ disease. Some documents (e.g., ASHRAE Guideline 12) included guidance, outlining specific preventive procedures.
The next milestone was the June 2015 release of ASHRAE Standard 188 which represented unprecedented agreement in the United States about the best approach to Legionella Prevention — implementing a water management program (WMP) for building water systems that can harbor and transmit Legionella bacteria.
“B” is not true, either. Legionella preventive information is available to building owners and managers, down to specific, detailed maintenance procedures and policies. Services needed to apply that information are available from water treatment companies, engineering firms, industrial hygiene firms, and consultants. Technologies for effective water treatment and filtration are also available.
Only a Small Percentage of Facilities Have Voluntarily Implemented an Effective WMP
If you have been involved with Legionella prevention, you know “C” is the correct answer to the above question. Despite government and industry warnings that building water systems must be properly managed to reduce the risk of Legionnaires’ disease — and guidelines to explain how — only a small percentage of facilities have voluntarily implemented preventive measures.
The anticipated spike in prevention from the release of ASHRAE Standard 188 turned out to be only a blip, even after the Centers for Disease Control and Prevention (CDC) published a report emphasizing “effective water management programs can reduce the risk of Legionnaires’ disease.”
Hospitals and nursing homes have begun to implement WMPs to comply with the requirement issued by the Centers for Medicare and Medicaid Services (CMS) on June 2017, but only a small percentage of hotels, apartment and condominium buildings, schools, college campuses, commercial buildings, and industrial facilities have WMPs.
Could ASHRAE 514 Increase Legionnaires’ Disease Cases Over the Next Few Years?
There’s no reason to believe facilities refusing to follow ASHRAE Standard 188 would voluntarily comply with the more burdensome requirements of ASHRAE 514 if it were to become a standard. Logically, voluntary WMPs would decrease if the perceived burden was greater.
Worse yet, simply working on ASHRAE 514 could delay voluntary implementation of WMPs by facilities. It happened before. A few hospitals started developing WMPs in 2000 after the Joint Commission announced a pending standard (finalized in early 2001) requiring health care organizations to develop a plan for “managing pathogenic biological agents in cooling towers, domestic hot water, and other aerosolizing water systems.” The number of facilities establishing WMPs continued to increase from 2001 until the first draft of ASHRAE 188P was released in 2010. Between then and the completion of ASHRAE Standard 188 in 2015, however, the number of facilities starting WMPs appeared to have decreased, likely because facility operators wanted to see what the final ASHRAE 188 document included before acting. The same could happen with ASHRAE 514 underway, particularly since busy facility managers pressured with tight budgets may welcome an excuse to procrastinate.
ASHRAE 514 could also delay state regulations. Right now, states could establish a simple principle-based regulation for all buildings other than houses, similar to the CMS requirement for healthcare facilities, requiring a WMP that satisfies ASHRAE Standard 188 (except with auditing of key performance metrics). But with ASHRAE 514 in the works, states may wait for it to become a standard before proceeding with regulations. Establishing regulations based on ASHRAE 514 could also require more work than a simple outcome-based regulation based on ASHRAE Standard 188 because of 514’s broader scope and more prescriptive content.
Since evidence indicates states hold the keys to the next step in Legionnaires’ disease prevention in the United States, a delay in state regulations is a delay in prevention.
What Will ASHRAE 514 Provide That ASHRAE Standard 188 Does Not?
According to ASHRAE (American Society of Heating, Refrigerating and Air-Conditioning Engineers), 514 will be built upon NSF 444, “Minimizing Risk of Disease and Injury Associated with Building Water Systems,” which was transferred by NSF to ASHRAE having never become an NSF standard.
Assuming, then, that ASHRAE 514 will be similar in content to NSF 444, the primary difference between ASHRAE 514 and ASHRAE 188 is that 514 will be broader in scope, aiming to reduce the risk of several waterborne pathogens rather than just Legionella, as well as physical (scalding) and chemical hazards associated with building water. 514 will require detailed, prescriptive WMP procedures, too, whereas ASHRAE Standard 188 essentially outlines only a framework of essential elements a WMP must include.
Yes, a good WMP should include control measures (design, operation, maintenance procedures) found to be effective in minimizing waterborne pathogens other than Legionella — while also protecting building occupants from scalding and harmful chemicals. However, WMP procedures adequately controlling Legionella will control most other biofilm-associated waterborne pathogens — very few additional control measures would be needed specifically for other pathogens. Requiring those few additional measures would be much more easily accomplished by expanding ASHRAE Standard 188 — already designated a standard in “continuous maintenance” — than by developing an entirely new standard.
A new standard (ASHRAE 514) should not be necessary to protect building occupants against physical hazards. The primary (perhaps only) physical hazard ASHRAE 514 would cover is scalding, which in most US states is already addressed, in part, by law. Most US facilities are aware of the scalding risk presented by hot water and are motivated to avoid the liability associated with it.
A new standard should not be necessary to protect building occupants against chemical hazards, either, since most or all control measures ASHRAE 514 would outline to protect against chemical hazards are already required by EPA regulations for chemicals added to drinking water or by plumbing codes for backflow prevention.
To the extent requirements to prevent scalding and chemical hazards are needed in a WMP standard, those measures could be added to ASHRAE 188.
If the benefit of ASHRAE 514 is to fill the ASHRAE 188 framework with detailed procedures, 514 would seem to be redundant with ASHRAE Guideline 12, which is being updated for that reason.
Is ASHRAE 514 the Right Idea at the Wrong Time?
Why are very smart professionals working on a standard (ASHRAE 514) aimed to provide more information if the rise of Legionnaires’ disease cases in the US is due to information ignored, not lacking?
Probably because they care. They want to see WMPs done well, done perfectly.
Swinging for the fence isn’t always the right play, though. More information at the wrong time — even if developed with good intentions — could increase disease or delay a reduction.
If ASHRAE 514 is a good idea, but for a later time, a faster path to prevention could look something like this:
- Require WMPs that satisfy ASHRAE Standard 188, auditing those WMPs based on a few simple but telling performance metrics, to relatively quickly achieve a major reduction in disease caused by Legionella and other building-associated waterborne pathogens.
- After most facilities have set up WMPs, develop an additional standard (e.g., ASHRAE 514), or expand ASHRAE Standard 188, to provide a broader scope or more prescriptive requirements needed to improve water management programs where audits have indicated gaps.
43 Years Has Been Long Enough
In the news now are 61 probable and 11 confirmed cases of Legionnaires’ disease, including one death, suffered by guests of a hotel in Atlanta. If the hotel water systems were the source of Legionella that caused the outbreak, an effective and fully implemented WMP based on ASHRAE 188 would almost certainly have prevented it. But until effective WMPs are implemented by facilities, Legionella infections will continue to occur.
In the 43 years since the outbreak at the convention of Legionnaires, researchers have done outstanding work in conducting studies to provide information and technologies for the control of Legionella in building water systems. It’s time to use it. Let’s not ignore or delay the real problem — implementation.
What do you think is needed to increase implementation of effective water management programs (WMPs)? What part, if any, should ASHRAE 514 have in that process? Please comment below.
I think your line of reasoning is correct. The problem is that many purchase WMPs and then fail to implement. From a conversation I had with someone involved with NSF444, they were some of the people that where kicked off ASHRAE 188 and didn’t think ASHRAE 188 went far enough.
Yes, some facilities set up WMPs but fail to implement them. As you know, our company is trying to make implementation easier, via LAMPS. I appreciate your efforts to help facilities, David. You’re doing good work. Thank you for commenting
My experience over the lasts 23 years is that even we have a very strict regulation since year 2003, we annualy have an average of 36 outbreaks, that affects an average of 1400 people a year.
The detection methods have improved, the inspections from sanitary authorities have increased, properties are investing a huge amount of money yearly and it remains allmost same in the last 10 years.
So I think the question is, that the goal is not to erradicate Legionella, as we should life with it, but to change the target, to control the Legionella the prevent big outbreaks.
Thank you, Jose. Yes, total eradication of Legionella is an unrealistic goal, but there is much evidence that the bacteria can be controlled to prevent cases of disease.
I’m a fan of 514. I currently hold several patents for a faucet that incorporates a mixing valve to prevent scalding. What people don’t understand is the current prevention method ( undercounted ASSE 1070 devices) actually promote the bacteria growth do to the problematic cross connections associated with check valves. If you provide a mixing valve above the “shut offs” you eliminate the ability to cross connect. This you don’t dilute the treatment method.
I think the reasons why Legionnaires disease has not decrease is due to both “B” and “C”. And the bottom line is that this is a business decision that will involve spending dollars.
The technology and the know how to prevent it is already available but if they have to spend thousands of dollars, they will take the risk.
I’ve just heard the news today that state of CA will allocate $150M to Improve potable water quality. This is a good start- the state and federal government should support the private institutions to tackle this problem.
Thanks Rey! I’ll look for the article about California funding water quality improvements.
It’s absolutely C. Until Building Owners and Managers are forced to budget for preventive maintenance and necessary testing to ensure that their steps for prevention are working then many will continue to ignore.
Thanks for commenting, Georgia!
The largest reason I hear from most of the contacts I have been attempting to get WMP’s for is there is nothing requiring them to do the program or a penalty if they do not. Most nursing homes and some hospitals are not doing this as they state they can’t afford the cost and they do not care if they get a fine. Most of the fines are very small and they just would pay it and go on without establishing a WMP. Until the State makes it a law and there is a large penalty applied to the owner of the building or facility and the State really makes an effort to uphold the law I do not think they will do anything.
Thanks for sharing the feedback you’ve received, Chuck. All facilities can implement the many control measures that cost essentially nothing. As technologies improve, the cost of solving the more complex problems should go down.
I think it should be a requirement to test building water systems all of them . like emergency eye and shower stations that are heated for example.
Thank you for commenting, Amy!
Well written, ASHRAE 188-2018 should be expanded not replaced. It is my opinion that NSF is still trying to corner the market and make everything run through their audit and approval process.
Keep up your good work, Mike! You’re helping a lot of facilities, which is impacting 1000s of people. Thanks for commenting
In my home state of Queensland (Australia) water management plans became mandatory for all hospitals (in 2017) and will be mandatory in all nursing homes within the next couple of years. The scope of these mandatory plans is similar to planned ASHRAE 514 and the WHO water safety plan model. We also have mandatory next day reporting of Legionella detections to the state Department of Health and publication of quarterly Legionella results for all regulated facilities on the Department’s web page.
Confirmed legionellosis cases from hospitals in Queensland are rare. Indeed, our state-wide incidence of legionellosis from Legionella pneumophila was only 0.5 cases per 100,000 population in 2018 (the majority of other cases being L. longbeachae which are not water related).
Two years into our regulatory framework compliance is improving, but much remains to be done. There is sufficient technical support available, through both the government and private sectors. But the reality is that some facility managers still do not take the risk seriously enough, at least until they have a case of legionellosis, by which time it is too late, and they have to suffer the consequences.
Water management/safety plans are the way of the future, certainly for all kinds of health care facilities that provide overnight stays. Extension to the hotel sector is also a worthwhile undertaking, but unlikely to be mandated in the immediate future in my jurisdiction. As for other larger building types, consideration of risks from building water systems should certainly be encouraged, but maybe as part of a comprehensive facility management system, rather than as a standalone water management plan.
I appreciate your comments, Greg. Although the article is mostly about standards in the US, it helps to get the perspective of a foreign health agency, especially Queensland since you have so much experience with Legionella regulations. Good job training your own personnel, too!
Experience in Germany is, that implementation of technical guidelines (DVGW W 551, first issued 1993) had been applied only by a limited number of building Operators, partly due to costs (e.g. regular sampling). Number of buildings checked for Legionella only increased dramatically after legal enforcement of Legionella sampling and measures to be taken in buildings exceeding a “technical measurement level” of 100 cfu / 100 ml. Legal enforcement has been issued in 2011 and since then we see a decline in buildings contaminated with Legionella. The framework is still laid down in technical guidelines, but legal enforcement of reporting results of Legionella sampling in buildings is the trigger to get building operators involved. Only since 2011 we see a still growing interest in application of technical guidelines, of course especially in buildings under pressure from authorities (e.g. proof of not exceeding the “technical measurement level” after correction measures in the building).
WMPs are still voluntary, but mandatory sampling “opens the door” to the buildings. To select sampling points first question is for the system documentation. It’s good to have a WMP implemented then….
Thank you for sharing the outcome of your guidelines and regulations, Benedikt. It’s very helpful to hear from officials in countries that have Legionella regulations. It’s interesting that you require sampling but not WMPs, holding facilities accountable for results but not the process. To my knowledge, your regulations prohibiting the use of chemicals is also unique.
Having worked in Legionella cure and control for 30 years now in the uk. I have found that if buildings that are run to a higher than any usable standard such as Ashrae then the control and prevention will be maintained
Thank you, Mark!
In answer to your immediate question, “What do you think is the primary reason Legionnaires’ disease has not decreased since the outbreak in Philadelphia…”, I believe that there is now dramatically increased testing for Legionella and that illnesses previously thought to be pneumonia, is not properly identified as Legionella.
Also, WMP are only required in health care facilities. When Legionella is identified in these facilities, it is quickly corrected and monitored. The bulk of Legionella outbreaks that I hear of , however, are in apartment buildings where WMP are either non-existent or virtually ignored.
I believe that ASHRAE 188 could easily be modified to include the intended inclusion in ASHRAE 514. This should include apartment buildings and other facilities in addition to Health Care Facilities. It doesn’t help to make new regulations when the old regulations are not widely enough used or when they are ignored.
Thank you, David!
We do yearly testing to verify that our PMs are working. When we first made our WMP there was not much info out there, but now it is fairly abundant which I appreciate. As for more stringent guidelines I agree with the points after this “If ASHRAE 514 is a good idea, but for a later time, a faster path to prevention could look something like this………….”
Kevin, it sounds like you had a WMP for your facility well before the CMS requirement, which is impressive. Good job!
The answer is always C. I have been on the front lines of this longstanding health risk. It has not been easy. Education is of great value. The LAMPS program is an exceptional tool for healthcare facilities.
Keep up your good work, Brock! Thank you for commenting
It is unfortunate that despite whatever standards are approved there will be management that will look for ways to get around them. Some People work very hard to address the standards and develop ways to work with them only to discover that management only gives lip service to the issue as they view the standards as a waste of time and money.
Thanks for your insight from a state health department’s perspective, Joseph. Even if regulations requiring WMPs per ASHRAE 188 are established, there will be some facilities that find ways around it. But most (97%?) will comply. The other 3% will never be reached. But 97% is better than what we have now (nil) for non-healthcare facilities with WMPs.
I agree that working on an entirely new standard only makes compliance with the existing standard more unlikely. My experience is that facilities that have a well-developed Water Management Plan have learned pretty quickly how to implement it. Continuous improvement of the standard and the plans written around that standard will certainly reduce the risk of Legionella transmission. I think that New York offers a good example of how state legislation can incorporate the principals of ASHRAE 188 effectively for reasonable and sensible regulation, even in the face of public and political pressure.
Thanks Rob! Yes, New York State has done a great job leading the way, as the only state so far with regulations. And, to my knowledge, they are looking at improving and expanding what they have.
I do not know the situation in America, but I wrote a publication about 206 buildings and the effect of the regulations in the Netherlands and these regulations do not prevent the grow of Legionella spp..
Science Direct
Thank you for sharing that, Wilco. I hope the link to the report appears in your comments because it will help us here in the US to know what form of regulations has been unsuccessful, at least in the Netherlands.
I agree that the information is available and that building owners/managers are not implementing this information. Unless it is required by law facilities do not want to implement WMPs due to the cost associated with the plan and then the additional cost/”burden” to implement the plan. We have even developed WMPs for facilities and then they aren’t followed or the facilities only want to do what is required by local regulations.
Thanks for sharing that, Jenny!
Matt,
I was involved with ASHRAE for Guideline 12 (the first one and with 188). We had a fearless
Chairman that did not want the Guideline or the Standard to be onerous as a Guideline,or Standard
or Code. It was to be effective and not overbearing. He vetted every member to be sure there was
not a personal or corporate agenda for any of us. He only wanted to benefit our industry, prevent
illness and death from LD. His name is Dave Geary and he should be graciously thanked for
his commitment and dedication to the original goals of the Guideline and Standard. It took us many years of ASHRAE meetings to develop the Standard and it’s purpose should not be diminished by personal gain, politics and power. Let’s help others and not ourselves.
Well put, Mike. And, yes, we own many thanks to David Geary and his work.
Our facility made the decision to utilize your system to be pro-active on this subject. I feel expanding and enforcing ASHRAE 188 would be a better choice.
Thank you! It’s good to hear from a facility that has taken action!
I agree with your statement that facilities will stop moving forward with a current plan if they think another plan is coming. Why spend the money on something now if I will have to redo it in the near future. By adding those new requirements to ASHRAE 188 instead of creating a new standard will allow facilities to continue on their current plan of implementation knowing they may just need to tweek the plan instead of recreating it. I also agree that the industry has spent so much time talking about it and not enough time implementing. I think that keeping the momentum moving forward with ASHRAE 188 would be a more effective solution to stopping the spread of water-borne illnesses.
Thank you, Tracy! And thanks for the good work your company is doing!
I have a friend who always says “Don’t let pursuit of the perfect get in the way of the good”. I feel ASHRAE could use this advice when it comes to 514. The beauty of 188 is its suppleness that allows it to be implemented in a wide range of businesses and institutions in ways that enhance best practices maintenance. Could an enhanced 12 help? Of course. We should remember that NSF444 was a flawed endeavor from conception and for ASHRAE to pick up the pieces on it seems a fool’s errand.
If one company drags their feet on a WMP because the are “waiting” for 514 and someone there acquires LP, what will will ASHRAE think then of this pursuit of the perfect?
I love the quote, Pat! Thank you for commenting
I have contacted a number of facilities in Montana and the response is basically why do we need to develop a WMP there is no requirement in the state for us to have one. Until the state and federal government made this a law with heavy fines most facilities will just take the risk.
An unfortunate result of living in a pretty heavily regulated society is the mindset that certain precautionary measures must not be needed if they are not required by law. Thank you for commenting, Bill
Our fearless leader, Dave Geary, for Guideline 12-2000 and 188 had a passion for these documents not be developed for any agenda, power or politics. He wanted to develop them to be effective for our industry, reduce illnesses and save lives. He questioned all of us and ASHRAE did reviews of the members frequently to make sure we were on the team for the right reasons.
I think this spirit should be renewed and continued with the integrity with which all of this was started in the early nineties.
Thanks for commenting again, Mike
My experience from the consulting engineering perspective is that it is both A and C. Since developing a WMP on a voluntary basis has been less than enthusiastically embraced in the built environment I believe a defensible conclusion is that there is a lack of agreement as to the risk:benefit ratio amongst building Owners and operators.
I do agree with the points made in the article regarding modifying the standard already in place rather than providing an additional standard.
Good point about the risk:benefit ratio, Hunter. I think many more facilities would implement WMPs if they understood the benefits versus cost. Thank you for commenting
Matt, I agree with most of your article. I think C is still the biggest lacking aspect — and it’s in the supermarkets, condos, hotels, and other facilities as you’ve indicated.
B is also still a factor due to plumbing codes in states, I would also argue, or resource hurdles due to lack of competition and mechanical contracting firms’ expertise (i.e. in the master spec).
But…it’s also in people’s homes. I tested my water in my previous home and found SG 1 present.
I think a larger issue is also the fear sites have currently of the AHJ’s that will point the finger at them, blast them to the news, and assign blame when, in my view, it’s circumstantial evidence at best.
Facilities definitely need to step up the game, no doubt. So too does the general public. Awareness and education vs. news bites and scare tactics are needed.
We won’t ever make water sterile. But if water safety is as common as fire safety — then we don’t just rely on the hospitals or hotels to notice smoke in our own homes. Or in the grocery store or Panera where I get ice.
I agree with too many standards will simply dilute the message, stretch resources thinner, allow for more predatory sales practices vs. real consulting as we do, and drag the process out.
It isn’t rocket science. It just takes work. A lot of it.
Yes, a cooperative spirit and hard work are definitely needed. If AHJ’s establish regulations to collect fines and burden businesses, we’ll end up with box checking instead of real prevention. A study of principle-based regulations for Australian nursing homes versus prescriptive regulations for nursing homes in the US sheds light on this. The outcomes of the simpler, principle-based regulations were much better. Kevin, I’ve heard you’re doing great work, helping a lot of facilities. Thank you!
Thanks for the excellent article. Implementing a successful WMP for legionella control takes more than just buying one… it takes a change in attitude about the responsibility for managing a facility. Adopting a public health centered attitude and implementing a WMP together would likely address other health risks in addition to Legionella control.
Ultimately, adding a new standard (518) when the old standard (188) is poorly implemented is rash. A new standard should build on lessons learned from implementation of the old standard. We have not learned any lessons yet, because implementation of 188 is poor, at best.
As a community, I believe our energy is best spent on efforts to ensure successful implementation of legionella control through 188 before we look to the next standard.
Chuck Cheatum’s comments get to the heart of it–there is a perception of large increased cost in implementing legionella controls, even though many parts of a WMP can integrate seamlessly with existing maintenance programs.
Meaningful enforcement would help. In the world of public water systems, fines are a secondary motivator to public notification. Should there be notification requirements for health-care facilities (and other buildings) that do NOT have a WMP? A big sign at the door saying “We do not protect your health from potential contact with legionella”?
I think that we need to be talking about the carrot (education, public health, safety) and stick (fines, public notice, etc.) for the existing standard before we build another standard on an unstable platform.
Thanks for the opportunity to comment, Alicia
Wise words, Alicia! Thank you for commenting!
Biofilms are root cause of pathogen risks in drinking water and Ice. I find it counter productive and unprofessional the way ASHRAE and NSF have behaved. This baloney degrades both organizations and calls to question the competence of members to develop a biofilm PREVENTION Std that in turn results in insignificant risk from infectious organisms and the risk factors that enable amplification and disease transmission.
At this point many health care facilities are in “must do mode,” which is really a reactive mode as opposed to taking a proactive approach to the prevention of disease. It is highly likely in my estimation that this will continue with the ultimate passage of ASHRAE 514. Both 188 AND 514 are very important measures, and I don’t know that the 514 “discussion” that is now taking place and will continue to take place will necessarily inhibit those taking action (especially health care) in adopting plans but may, unfortunately, inhibit the implementation of those plans
Thanks for commenting, Tom!
I think the NSF has much to offer. I would be carefull in excluding anything that does not appear to immediately reduce the amount of LD outbreaks. Legionella has so many unknowns. Codes follow standards, but state governments and their health departments have enough information to put preliminary legislation in place to start mitigation. The exact science of water sampling and testing is still evolving. And that’s the most important validation of a WMP. We should be carefull in setting standards and codes that may miss important items that may come back to haunt us in the future.
I still believe public education is key. The more the building inhabitants know about legionella and LD the better the chance of action. Owners will have a tougher time avoiding the hard questions of their customers, if I can use that term to describe people who live, work, play, learn, eat, sleep and receive healthcare in any respective building.
Yes, education needs to continue no matter what’s done to bring implementation of WMPs. We need to keep researching and learning. Thanks Manuel
I agree with your thoughtful analysis, and also think that updating ASHRAE-188 is a better approach than creating another standard. On behalf of someone in the regulated community, it gets very confusing and frustrating when you have multiple regulations with overlapping purposes- many of us are stretched thin and would prefer to have one regulation/standard we know we can rely on as best practice.
Thank you Becky! And thanks for your hospital’s good work
Before creating more voluntary standards, perhaps our time would be better spent working with law makers who could take standards like 188 and make them requirements. This would absolutely save lives and reduce disease. How many people would drive around without automobile insurance if it wasn’t required legislatively. I bet its the same with WMP’s. Until its required, most people will not implement a Water Management Program.
Thanks Tom!
I agree with you, Matt. Thank you for this excellent article.
Thank you, Greg!
Great article Matt and some really good thoughts. As an attorney my experience has sadly been that all too often owners will only develop WMPs once there is an outbreak and/or potential litigation. I do not think that adding another standard such as 514 will result in any motivational change to this fact. In addition, even the owners that have WMPs in place frequently do not implement the plans and only have them because it was a requirement to “check some box” in order to obtain insurance or comply with some inspection process. Incentives or penalties might help in getting owner to develop WMPs but still will not guarantee implementation. Even in cases of litigation- years after settlement- compliance wanes.
Thanks Russ! It’s good to get your insight from litigation experience.
I believe that a properly implemented WMP following guidance from ASHRAE 188 not only helps to control and prevent Legionella, but sets standards and practices that are effective at controlling other pathogens as well. While 514 may enhance and improve upon 188 it is also likely to create confusion in the industry and reduce the number of voluntary participants that follow ASHRAE 188. A more common sense approach is to continue to improve and expand 188 to include more and better practices for increased pathogen control.
Thank you for commenting, Richard!
Great article Matt! I agree that it is likely that we are perhaps taking our eye off the ball a little bit with ASHRAE 514 in lieu of ASHRAE 188, and I do think that a WMP is definitely part of the solution. I think we should focus on Legionella first while acknowledging that other risks are there as well.
That being said, I disagree that “A” is no longer an issue – in my mind it is the biggest issue. ASHRAE 12 unfortunately does not provide specific enough actions to mitigate risk from a plumbing design perspective. Most efforts to mitigate risk are based on post-construction activities, and all the factors such as outdated sizing methodologies, low-flow fixtures, and not understanding the uses of new technologies are not being addressed. In my mind we need a much more concerted effort on addressing the disease of “bad plumbing design” rather than only the “symptoms of mitigating outbreaks with a WMP”. I do not think changing plumbing design wholescale will fix 100% of the issues, but WMP’s alone will not address this challenge – it really is a marriage between the two that will help minimize this disease. Until plumbing design is wholescale addressed, we will be only chasing our tails.
Thanks for commenting Christoph. Specific measures for designing plumbing systems to minimize favorable conditions for pathogens definitely needs to be part of WMPs. We have about 40 specific design/construction control measures in our LAMPS WMPs, many of which pertain to domestic water systems. The information is definitely needed. For years, though, ASPE has been providing information (I taught a full day seminar on plumbing design for ASPE in 2006) that many plumbing engineers have not applied. Thank you for doing so much to increase Legionella awareness among plumbing engineers. Keep up the good work!
ASHRAE 514 will not increase Legionnaire’s Disease (LD) rates. The LD rates have gone up because diagnostic and reporting rates have increased. LD has been with us since we started using water for drinking, bathing, sanitary, heating and cooling purposes.
I choose reason C. We have the technology and know how to recycle wastewater into drinking water on the International Space Station. We have only implemented a small fraction of this capability. Is a water management plan worth it? Depends on who you talk to. A building manager who has never had any LD cases traced to his building will tell you a water management plan is expensive. The owner of hotel who caused an LD outbreak and is sued into bankruptcy will tell you a water management plan is well worth the investment. ASHRAE 188 is sufficient. No need to duplicate efforts with ASHRAE 514. Work on making 188 better. The 24/7 news programs on TV and the internet will drive LD awareness and drive water management programs. We are now aware of an LD outbreak that occurs next door as well as thousands of miles away.
You’ve made some good points, Dan. Better and more widely used tests to diagnose Legionnaires’ disease may help in convincing building managers that WMPs are worth the cost, by revealing more undiagnosed cases. Thanks for commenting
A good provocative piece on the prospect of a new more stringent standard for water safety. There is always a balance between prescribing a strict enough standard that it’s effective and creating something that seems so costly and time consuming that industry players balk at implementation.
The simplest solution is for regulators to create a cost for non-compliance. That cost can be both monetary as well as reputational. As you mention, the key to this seems to lie with states.
Thanks Eliot!
ASHRAE 188 and 12-2000 Revision is more than enough standards and have been promoted for inclusion in codes for many years. If ASHRAE wants to incorporate NSF444 into the standard or guideline that seem appropriate to update accordingly. Introduction of a totally new standard will create more confusion in the marketplace.
Commercial buildings do not seem to understand that it is their responsibility to implement a WMP that includes proactive treatment. Everyone is fully aware that Public Water Supplies contain Legionella and other pathogenic organisms that can contaminate their potable water and non-potable water systems. However, these facilities that purchase “City Water” fully expect the water to be safe for its intended use and are shocked to find out they have an issue in their building.
Education vs regulation needs to be made available on not only development of a WMP but proactive treatment. Most of the WMP that I speak very little to treatment. Chemical solutions such as secondary disinfection are not controlling the problem as the hot water and bio film conditions quickly consume the residual disinfectants.
Secondary filtration to remove the dirt and microbial contaminants entering the building and filtration on the hot water loops will greatly reduce the problem without secondary chemical disinfection. Especially since the State Primacy Agencies regulate these facilities when they do install secondary chemical disinfection further increasing the cost to these private facilities.
Validation for the health of the premise potable and non-potable water systems is critical to verify that the WMP is working. With new Legionella testing coming to light the day of culture tests seems numbered. DNA extraction type PCR test seem more accurate and faster, while not necessarily lower in cost.
These new test methods need to be included in any revision to ASHRAE 188.
Thanks for taking the time to comment, Andrew
Keeping things simple and straightforward makes it easier for those who want to comply with WMP requirements to comply and limit the excuses for those who are not interested in complying. Creating a new standard like ASHRAE 514 gives building owners and managers an excuse for not implementing a WMP and prevents regulators from implementing regulations. Water Management Plans work when they are implemented and are already helping to control other waterborne pathogens such as Pseudomonas targeted by NSF 444. By expanding the ASHRAE Standard 188 it keeps things simpler and more straight forward for the people who are implementing the plans on a day-to-day basis.
I appreciate your comments, Brady!
For me the answer is simple: lack of top management responsibility. The disease are not easily diagnosticated, and time/local are sometimes difficult identify, e.g if you only have a few cases (2 or 3), (and if this cases dont reach the press :-)), it is very difficult to prove “on time” a cause/effect and investigate all the scenario (…local, and a responsable). So the thing is, rules must be fulfilled, ASHRAE 514 is a step forward and once again top managemet responsability is the key.
Thank you for commenting, Rui
In Québec Canada, hospitals rarely have WMP because they don’t have a budget to pay for it. We have a regulation for cooling towers only but it is not well respected because there is little enforcement, no funding and the perception of little risk.
Thank you for sharing that perspective, Valerie. Coincidentally, just this morning our support team received an inquiry about LAMPS WMPs for facilities in Canada, and particularly in Quebec. My understanding is that most facilties in Quebec are simply trying to comply with cooling tower testing regulations rather implementing comprehensive WMPs. Your comments help us better understand the challenges and position of facilities in Quebec. Thank you
Well written article, Matt.
C is definitely the right answer. There is plenty of information available, but as long as building owners do not understand why they need a WSP, they do not want to spend the money for it. ASHRAE 188 is sufficient, if people understand the content. In the food and beverage industry, they understand the need, as consumer safety is critical. Many years ago we (I) decided to look at water as food. We have been using ISO 22.000 (HACCP Hazard Analysis and Critical Control Point) as frame for our WSP for technical water installations (adiabatic humidifiers) since year 2001. ASHRAE 188 recommends using exact same methodic as described in ISO 22.000. The main difference is that 188 only deals with Legionella, where ISO 22.000 covers all risks involved, including chemical and mechanical risks. Again – as long as it is not mandatory, people will only implement a WSP if they understand why it is needed (or required by law). Training, training and training….. This is my experience after 30 years of work with engineers and technical people – not used to work with microbiology. Reason? You can not see bacteria or measure them as you can with temperature and pressure etc. When we develop new adiabatic system, within our organisation, risk assessment and the necessary maintenance and cleaning instructions to ensure a safe system are required and evaluated before any release is allowed.
Philosophy for Technicians: When you know why – you will know how.
Thank you for commenting, Leo. Good point about the importance of training so that maintenance personnel know why, not just how.
From my perspective, I see a needed change in your options.
This is your
B. Information, services, and technologies needed to control Legionella in building water systems are not available to building owners and managers.
Which I think should be:
B. Building owners and managers are not fully aware of the available Information, services, and technologies needed to control Legionella in building water systems.
And then the answer would be both B and C because for the ones that are aware and do not fall in B then they fall in C. But still way too many in B!
Having stated that, although I had not given thought to 514 in the perspective that you are raising, i.e.: that it could slow down implementation of WMP.
I certainly feel that at this time, 514 is not needed and better diffusion of and insuring more regulations linked to, ASHRAE 188 should be the focus of all interested in lowering both Legionella and water borne pathogens risks! That in and of itself to me will also address the scalding issue that is an additional aspect that 514 is supposed to address.
Keep up the good work!
Thank you for commenting, Alain. Good point about the awareness versus availability of information. It’s surprising but true that many facility managers are still unfamiliar with the risk of Legionnaires’ disease and the need and means to prevent it by controlling Legionella in building water systems.
I think the answer is C from a South East Asian perspective. I live and work in Goa , India, which is on the Global tourism map , and i am surprised to note that few branded star hotels budget for preventive maintenance and necessary testing to ensure that Legionella infection is prevented in their Water Systems . Going forward , the need of the hour is bring about strong legislation for implementation of the Standard 188 -2018 which already has the support of ANSI in the USA and perhaps work on making it more inclusive to incorporate some of the NSF 444 guidelines at this time, rather than initiating work on a whole new Standard 514 .
Thank you, Mahesh! We appreciate your perspective.
Let’s start by going back to the original question: “What do you think is the primary reason Legionnaires’ disease has not decreased since the outbreak in Philadelphia [ 1976]?”
A better question to ask is why has there been such a dramatic rise in number of cases? Here are my answers- note that I believe it is a combination of items listed below:
• Reporting artifact- more attention has led to more patient testing & reporting of positive confirmed cases
• Aging infrastructure affecting plumbing
• Increase in water conservation practices
• Inattention to routine maintenance of H20 distribution systems
• Outdated plumbing codes
• *Lack of qualified 3rd party consultants with specific experience in dealing with Legionella bacteria in water distribution systems
I disagree with this statement because ASHRAE 188 is not “the best approach”, it is one of several approaches that can be effective if followed:
“…ASHRAE Standard 188 which represented unprecedented agreement in the United States about the best approach to Legionella Prevention — implementing a water management program (WMP)…”
“Only a Small Percentage of Facilities Have Voluntarily Implemented an Effective WMP”- The national emphasis has been on healthcare facilities. If we want to engage other types of facilities, then new educational and support campaigns are needed to reach them. For example, if we want to get hotels on board with having WMPs, then we should design a campaign for the travel industry that takes into consideration how this industry works, and, importantly, how they are or are not regulated. I can see incorporating material about WMPs into university curricula aimed at individuals going into hotel management.
I think the original question is asking if people think that we need another standard (something more prescriptive than ASHRAE 188)? Personally, I look at 188 as a framework, but certainly not the end-all be-all). My experience has shown me that healthcare does not understand how to use it, and that clients want to be told step by step what to do. So, do we need a new std? Probably, however…
What we absolutely need is an accessible 3rd party consultant workforce that is highly trained in the specifics of dealing with Legionella and other opportunistic plumbing pathogens in water distribution systems in the built environment. For the most part, we do not have this now. There are precious few consultants that have the depth of knowledge and experience needed to work with facilities to set up routine programs, and even fewer who know what to do in response to an identified outbreak. Facilities need outside help to show them why their building has become an incubator that allows low concentrations of naturally occurring organisms to now multiply, travel, and colonize parts of the building’s water distribution system. For most of these facilities, we advise them to hire a 3rd party consultant. The LAMPS program is an excellent program for facilities that may wish to take on some of the work, but needs guidance and assistance for either discreet pieces of the WMP or an assist with the entire program. LAMPS provides incredibly useful analytics based upon the client’s own data. This allows the client to review their own data and make meaningful changes to their WPM that reflect what is going on in their own buildings.
In conclusion, I believe that for any standard being used, it is critical to have an educated workforce that can help facilities construct a functional WMP, put that WMP into play, and provide continuing review and modifications of that WMP. Without these pieces, the number of cases will continue to climb and all of our efforts in protecting the health of the public will be severely hampered.
Marian, thanks so much for taking the time to add thoughtful comments. It’s helpful to have the perspective of a state health department. To clarify, the statement about ASHRAE 188 representing unprecedented agreement about the approach to Legionella prevention in the US was in reference to implementing a WMP. My understanding is that most experts agree, as I think you do, that facilities should implement a WMP. Opinions vary, though, as you pointed out, about the detailed procedures a WMP should include. Yes, education is definitely needed. HC Info is trying to do our part in that by making LAMPS available, not only to facility end users, but to the companies that provide services to them. I think the companies that have gone through our training to become authorized LAMPS WMP providers are doing an excellent job in training their personnel, setting up WMPs for their facility customers, and encouraging ongoing implementation. Thank you for being a leader and influencer among health departments, setting a good example by having become so educated yourself on Legionella prevention.
Lack of knowledge is normally always the factor.
It is my goal as a water treatment provider to teach my customers of the dangers of not properly treating and controlling their facilities different water sources.
Thanks for your efforts, Bryan, and for commenting
I will limit my comment to Cooling Tower Systems. I wrote a 36 pages book on the subject: “Wake Up and Avoid a nightmare”. As you Matt, I think that, after 43 years from the time when Legionnella was identified, the fine word is ACTION. Knowledge is there. What is missing is the will to implement it. In the book I explained that a paradigm is widespread even by a manufacturer. A warning sticked on Cooling Towers states : regular maintenance and biocidal treatments are necessary. Consult a water treatment expert.” However, we all know that outbreaks occurred to Cooling Tower Systems having biocidal treatments and maintenance program. There was the case of the outbreak of Quebec City during the Summer 2012… So, the important point now is to shift to a new model or paradigm and implement it. ASHRAE Guideline 12-2000 and ASHRAE Standard 188 both lead to minimizing or managing the risk to transmit LD. I repeat it. Time is not to seat down for years to come but to stand up, get into ACTION, go where is the need and implement an efficient Risk Management Program.
Thanks Mario! I look forward to reading your book.
If you look at data from the CDC, we can see that the cases of Legionella in the country are rising dramatically. With an aging population combined with other factors like a warming climate that will put more emphasis on cooling systems, there is every expectation that this trend will continue unless we pay better attention to the environmental sources.
Thanks for commenting, Norman
As a field health practitioner in Queensland, Australia, I believe prescriptive legislation is necessary to ensure mandated Water Management Plans are implemented, and the owners of the plan held to account. Since the regulatory changes occurred here, it has been my experience, in health facilities at least, that the people responsible for the plans are taking negative legionella test results seriously, and tend to welcome assistance with planning and implementing remedial measures. Whilst in its infancy, I see the new regulatory framework as a key tool in preventing legionella cases in the future.
Very helpful, Paul. Thanks for sharing the results so far in Queensland.
Standards and Guidelines, no matter how good they are, which are not enforced by Legislation are next to useless as their implementation is subject to individual enterprises’ priorities and circumstances. Costs will frequently decide to what extent the Standards will be adhered to.
No Standard or Guideline will cover all aspects of Legionella control, now or into the future but unless they are forced on firms to implement with fines imposed by local Authorities, these Standards and Guidelines will never improve. Frequent Testing and reporting of legionella detections will provide feedback information to building owners and occupiers on whether their Water Management Plan is effective in controlling legionella. The statutory reporting to authorities if Legionella is detected will ensure that follow up action is taken.
Legionella testing is not a control method but rather a warning sign that the WMP needs reviewing.
Expertise to improve aspects of individual WMP may not be available “in-house” and hence there is a need for private firms or government instrumentalities to be available to provide that assistance.
Thank you Michael!
Thank you for the excellent article. I absolutely agree with you. From my observation and talking with building engineers, keeping up with the Water Management Plan is a lot of work and attention to detail. Providing the wrong data or missing information from the WMP can be costly (I’ve seen violations total up to $10,000). Depending on the building, some engineers may need to receive extra attention to make sure they are maintaining the WMP properly. Of course, the larger the team of engineers, the easier it is to manage the program. If there are new standards that compound with the original standard developed, there will be resistance among engineers in NYC. Plenty have already given me the “I do not have the time to manage my WMP” and are only willing to do so because it is law and do not want to pay the fines. I believe that unless there are actual laws in other locations other than New York State, building owners and engineers won’t insist on preparing a WMP to manage Legionella especially if they are aware of any new changes to the current standard or a new standard in its place. I think for now, we should keep it simple and base our WMPs on standard 188 and not complicate the matter further until more WMPs are developed within every building that utilizes a water system.
Keep up the good work you and your company are doing, Matt! Thanks for commenting
First off: Thank you Matt for publishing such a thought provoking blog which, has resulted in a lively discussion of such a serious public health issue facing our engineered infrastructures. I 100% agree that the primary reason Legionnaires’ disease has NOT decreased over the years is because building owners and managers have not implemented the information, services, and technologies available to them to control Legionella in building water systems. Likewise, I also would 100% agree that only a small percentage of facilities have voluntarily implemented an effective WMP. And finally, I also find myself in accord and agreement with most comments and key discussion points posted thus far. However, while I tend to agree that a delay in state regulations might indeed result in a delay in prevention, I’m not (yet) completely certain, or ‘sold’ on the concept, that the STATES hold the keys to the next step in Legionnaires’ disease prevention in the U.S. Instead, I think it’s the FEDERAL government which holds the keys, and here’s why. It was neither the NYC nor the NYS Legionella codes, regulations, requirements enacted in 2015 which impacted other states, as much as it was the long-awaited and highly-anticipated final publication & promulgation (also in 2015) of ANSI/ASHRAE Standard 188-2015 (now 188-2018) Legionellosis: Risk Management for Building Water Systems, which caught the attention of the rest of the nation outside of New York. Couple that with the CMS S&C memorandum(s) of 2017 and the QSO revision of 2018, and the updated 2019 AWT Position Paper & Guidance Document, the 2019 OSHA revisions, along with the soon to be released NASEM report, AIHA update, and Guideline 12 revision, and we finally have something with not only broad appeal, but more importantly, broad applicability. Truth-be-told, the #1 comment I hear outside of NY is: “NYC/NYS Legionella laws don’t apply here in the State/Commonwealth of XYZ.” However, ASHRAE applies, OSHA applies, CMS applies (if they’re accredited healthcare), etc., universally across the nation.
IMHO, the last thing we need is a patchwork quilt of diverse and sometimes even conflicting state regulations. Heaven knows we already have that going on right now with EPA SDWA primacy, and how each different state (and sometimes county or municipality) interprets, applies, and/or enforces it within their respective jurisdictions; not to even mention that <2 dozen states even require schools (arguably our most vulnerable population) to validate compliance with the lead copper rule. Even in New York simply with Legionella, there are dozens and dozens of conflicts between the requirements stipulated in NYC Title 24 Chapter 8, vs NYS Sanitary Code 10 NYCRR Part 4; so much so that 100% compliance with one does not result in full compliance with the other. Therefore to me, the key is FEDERAL enactment of a standard which will alleviate confusion. If not that, then at the very minimum, something with broad reaching appeal, which brings me to ANSI/ASHRAE.
ANSI/ASHRAE 188 is a standard which concerns itself primarily with Legionella. It defines itself as establishing the minimum legionellosis risk management requirements for building water systems. That's it.
ANSI/ASHRAE 514 by contrast however, is anticipated to result in a safety standard which will concern itself with not just Legionella, but many other emerging waterborne pathogens, as well as the physical and chemical characteristics of building water systems. One has only to remember Flint, MI to see that something like 514 could've potentially helped in a situation or scenario such as played out there. ASHRAE has stated that the 514 development committee will not only be closely coordinating with the 188 committee, but will also be ensuring that there is no conflict or duplication between the two different standards. Therefore, I don't think there will be a resultant "either/or" implementation conundrum between the two, because they will be entirely different animals, established for entirely different purposes.
By virtue of their ANSI status however, the common-bond between the two standards will be their broad nationwide (even international) appeal, acceptance, and (hopefully) implementation.
Dominick, thanks for taking the time outline your opinions so well. I agree that if each state established regulations with different WMP requirements, it would be so burdensome to owners of buildings in multiple states, and to companies like yours that provide services in multiple states, that compliance would fall short and thus the outcome would not be optimum. For maximum prevention, regulations must be consistent for all buildings, at least throughout the US. For that to happen, regulations would need to come from a federal agency, as you suggested, or from state agencies that all use the same national standard. I appreciate your comments and the good work you do.
Hi All – From an African perspective all three points are applicable(but mostly C – as we aim to implement best practise with the use of international standards and guidelines). In addition we are lacking case statistics from infections related to public health and occupational health. Ecosafe’s Legionella sampling results over the pass 11 years presents a contrast to case statistics in South African, many detected/ out of spec Legionella results across all building / facility types.
Thank you for commenting, Jay!
I find much of the problem with WMPs is there are not qualified people that are preparing WMPs. There was an effort at one time to Certify People as Legionella Risk Management Professionals to assure they understood all of the areas associated with management of Legionella bacteria growth in building water systems. This requires a significant understanding of the following areas of expertise:
1. Knowledge of Water Chemistry & water testing methods for EPA Safe Drinking Water Act (SDWA) limits.
2. Knowledge of Disinfectant Chemistry (Water treatment chemicals approved for Drinking Water Systems per SDWA)
3. Knowledge of Microbiology and temperatures effects on microbial/bacterial growth (growth temps., dormant temps., kill temps).
4. Knowledge of Chemical effects on microbial/bacterial growth. (Levels for no effect on growth, control levels, kill/disinfect levels)
5. Knowledge of piping, valve and equipment materials and how the mechanical systems were designed to operate.
6 Knowledge of Plumbing system engineering design, troubleshooting, installation and operation/maintenance.
7 Knowledge of HVAC/Mech. system engineering design, troubleshooting, installation and operation/maintenance.
8 Knowledge of Process water system engineering design, troubleshooting, installation and operation/maintenance.
9. Knowledge of the effects/rate of corrosion with piping system materials exposed to various levels of water treatment chemicals.
10. Knowledge of the effects/rate of various levels of water treatment chemicals on humans (Carcinogens, toxicology, safe levels per EPA SDWA).
11. How to look at a piping system and draw an actual “Flow diagram” showing all pipes, valves, branches, dead legs, equipment and components in the piping system without using generic balloon diagrams.
12. Ability to analyze a system by looking at the system or reviewing the flow diagram to determine if the system is operating to control Legionella bacteria growth with temperature controls according to industry standards & codes.
Ron George (734) 755-one908
Training and experience are definitely important, Ron. The new ASSE/IAPMO/ANSI Standard 12080 “Professional Qualifications Standard for Legionella Water Safety and Management Personnel” is a huge step in the right direction. States that establish Legionella regulations may require individuals setting up water management plans (WMPs) or providing other Legionella-related services to become a certified “Legionella Water Safety and Management Specialist” per ASSE 12080. For example, if it becomes law, pending Pennsylvania Senate bill 1285 will require ASSE Legionella certification for individuals collecting samples for Legionella testing. Thanks for commenting, Ron, and for all you do to increase Legionella awareness.